
Leg Artery Disease in Women
Leg Artery Disease in Women: Symptoms and Treatment Options
The risk of leg artery disease, also called peripheral artery disease (PAD) is increasing. This is especially so with increasing levels of diabetes and obesity. Other important risk factors are age, smoking, cholesterol levels, blood pressure, kidney disease and depression.
Being female, or identifying as female gender to a lesser extent, has its own set of risks for developing and treating PAD. These risks include the effect of menopause on arteries, different experience of PAD symptoms, generally poorer risk factor control and contacts with health systems.
Overall, PAD is more common in men at first but over time, women catch up to men and will overtake them.
Why are Women Different?
Biology and hormones play a major role. Before menopause, oestrogen, and some other factors in the walls of arteries, have a protective effect against PAD. As a result of this effect, women tend to get PAD about 10-20 years after men. After menopause, this protective effect is lost and, overtime, women catch up to men. Women then overtake men because they live longer.

Women who have PAD are much less likely than men to have symptoms, such as leg pain on walking, also called intermittent claudication. When women do have symptoms, most will still have claudication but are also more likely to have atypical symptoms. These may be confused with arthritis, back pain or nerve pain. As a result of this, women often first seek medical advice when their symptoms and PAD are worse.
Also, if women smoke, they are less likely to be able to stop smoking. Control of other risk factors, such as obesity, high blood pressure, cholesterol, kidney disease and diabetes, is also less optimal than for men. Some of this may relate to gender influences in society, such as roles, expectations, marketing and social media.
Trans-females are subject to many of the same society and gender role influences, even if the addition of oestrogen therapy in this group provides some protection against PAD.

What about smoking when talking leg artery disease?
It is worth noting that smoking is by far the biggest risk for developing PAD, in both women and men. Smokers are, on average, seven times more likely to develop PAD than non-smokers. Research shows that, on average, it is harder to get women to stop smoking than men, even after going on courses to help a person give up smoking.
Diabetes and leg artery disease?
In women who have not yet gone through menopause, having diabetes cancels out the protective effect of oestrogen on arteries. One of the reasons for this is that high levels of blood sugar change the lining in the arteries, which in turn causes artery disease to progress faster.
Cholesterol?
A high cholesterol level increases a person’s risk of PAD. In women who have gone through menopause, cholesterol levels tend to rise once the protective effect of oestrogen lowers. Of interest, taking hormone replacement therapy (HRT) does not seem to reduce this risk. However, cholesterol-lowering medications, called statins, do reduce this risk in people who already have PAD.

Kidney Disease?
People with kidney disease are prone to more rapid development of PAD. This is a result of damage to the artery lining, which causes inflammation and progressive PAD. More women live with chronic kidney disease. This is probably owing to the longer life expectancy of women.
Depression?
Women are more at risk of depression than men. Depression increases the risk of PAD and causes reduced walking ability and more leg symptoms after treatment. Studies show that depression is one of the strongest stand alone risk factors for PAD in women but not in men.
Treatment Differences in Women with Leg Artery Disease
The first line of treatment for PAD is often stopping smoking, increasing exercise, eating healthily and optimising medications. Research shows that women are slower to get all of these treatments in place. Maori, Pacific Peoples and women in lower socioeconomic groups are more vulnerable.
Women have smaller arteries than men. This may lead to more complications with minimally invasive stent and surgical treatments. These include bleeding, artery blockages or infections. Once the treatment has been done, the longer-term outcomes are similar between women and men.

What is Thoracic Outlet Syndrome (TOS)
Thoracic Outlet Syndrome: Symptoms, Causes and Treatment
The arm vein, artery and nerves all pass between the collar bone and the bone of the first rib. When one or more of these gets compressed between these bones, people can get vein or artery blockage or nerve numbness, weakness or pain. Thoracic Outlet Syndrome (TOS) tends to affect young active adults. Diagnosis and treatment are important in order to reduce the chances of lifelong problems.
There are three types of TOS – arterial, venous and neurogenic. The artery type is less common compared to the vein and nerve types.

Venous thoracic outlet syndrome (VTOS)
Venous TOS is mostly seen in young adults who do a lot of repetitive overhead arm movements. These may be labourers, gym-goers who do weight training or swimmers. It will usually affect the dominant arm. In some people there may be an underlying blood clotting problem but this is not usually the case.

Another term for VTOS is Paget-Schroetter syndrome.
The features of VTOS are similar to those of a deep vein thrombosis (DVT) in the legs. Sudden onset of arm swelling, with blush discolouration is common.
Arterial TOS (ATOS)
Arterial TOS is mostly caused by extra neck ribs or extra fibrous tissue in this area that compresses the artery. Over time, the artery may block off or sometimes grow bigger and form an aneurysm.
Extra neck ribs are also called cervical ribs. About 1% of the population has these. They are more common in women.
ATOS relates to artery blockage, or to artery expansion, and is also called aneurysm. Artery blockage can cause either sudden or gradual poor blood flow to the fingers, hand and muscles of the arm. Aneurysm can cause a noticeable pulsating lump above the collar bone.
Neurogenic TOS
Neurogenic TOS is by far the most common type. It typically affects adults in their 30s and 40s. Extra neck ribs and fibrous tissue can be a cause but neck trauma from falls and vehicle accidents would be the most common underlying cause.
The features of NTOS relate to nerve problems affecting the arm, causing numbness, tingling, weakness and pain.
How is Thoracic Outlet Syndrome diagnosed?
Diagnosis is usually based on a patient’s arm symptoms, along with a number of tests. Often many of these are used in combination to get a clear diagnosis.
X-rays can look for extra neck ribs or any other bone problems.
Ultrasound scan can look at the veins and arteries in different positions to see whether there is compression. This is not completely diagnostic because about 25% of normal people get compression when the arm is placed in certain positions but ultrasound can easily detect blockages and aneurysms.

CT and MRI scans can give information on the vessels, nerves and spinal cord, muscles, bones and joints. Nerve impulse tests can work out where a nerve is being compressed.
What are the treatments for Thoracic Outlet Syndrome?
In some people, if a vein or artery blocks off causing only minor symptoms, no further treatment will be needed. This is also the case with minor nerve symptoms. Avoiding the repetitive actions that initially caused the problem is advisable. For vein blockages, blood thinners may be necessary for a period of time.
When treatment is necessary, the general aim is to treat the specific vein, artery or nerve problems and then to create more space for these structures as they pass between the collar bone on the first rib. Usually, a combination of X-ray techniques, such as stents and surgery can clear blood vessel blockages. Surgery can fix blocked arteries, aneurysms and clear fibrous and scar tissue from around the nerves. Also, removing the first rib, and any extra neck ribs, can create extra space and remove the compression on the vein, artery or nerves.
And the results of treatment?
Treatment results for vein and artery problems are predictably good. Many patients will have significant improvement.
Results for those with nerve problems are much less predictable, because some patients in this group may have had the problem for many years. Many will have chronic pain syndromes. So a multidisciplinary team of vascular surgeon, neurologist, pain specialist, physiotherapist and psychologist offers the best chance of a good result. Consequently, about 10% of NTOS patients will need surgery to free up compressed nerves and open up the space between the collar bone and first rib.


What are vulval varicose veins?
What Are Vulval Varicose Veins? Symptoms and Treatment Options
Vulval varicose veins affect the vulva, labia and perineum. For many women, they start in pregnancy and may either improve or get worse after they’ve had their babies.
In some women, the cause may be conditions that do not relate to pregnancy, such as blood clots (deep vein thrombosis (DVT), abnormal vessels or mechanical conditions that can cause compression of veins by surrounding structures, such as arteries. May-Thurner Syndrome is an example of this type of condition.
Until recently, exactly how blood flows within the pelvic veins has not been well understood. In particular, how the venous pelvis blood flow changes in pregnancy and how it goes back to normal, or not, after pregnancy.
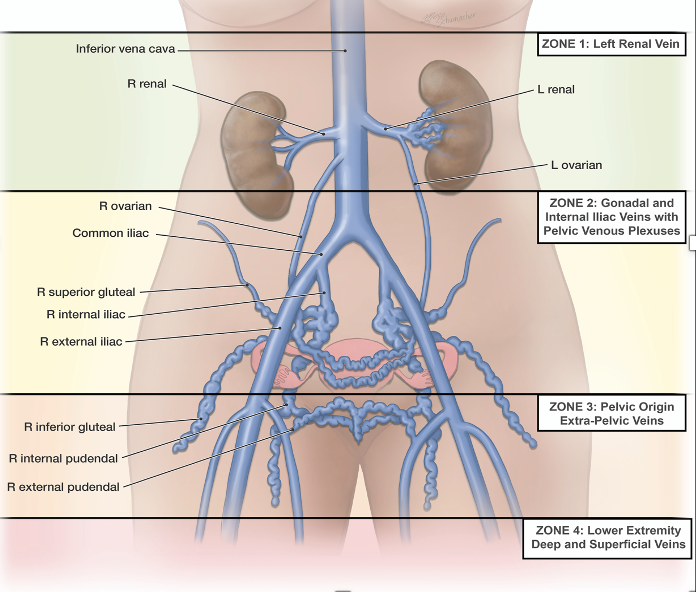
Venous blood normally flows back to the heart in one direction from the leg veins. In the pelvis, blood can flow in different directions before returning to the heart. Pelvic blood flow like this can allow ‘escape points’ or detour routes between the pelvic veins and the veins of the labia and vulva, causing varicose veins in these areas. Often, they first occur in pregnancy and may also continue after giving birth.
Four percent of pregnancies get vulval varicose veins
As a result of the ‘escape points’ between the pelvic and vulval veins, about 4% of women will get vulval varicose veins when pregnant.

The pelvic veins can also communicate with veins in the legs. These include veins around the buttocks, the lower abdomen, and upper inner thigh area.
Ultrasound scanning is usually the first investigation for working out the cause of these veins. Sometimes transvaginal ultrasound will be useful in assessing the pelvic veins. Ultrasound scan will be performed standing or half standing, half sitting. CT and MR scans may also be very useful for diagnosis.
What are the Symptoms?
Vulval varicose veins cause aching, throbbing, heaviness, pressure and a feeling of fullness. Commonly, symptoms worsen with periods, exercise and on standing and sitting. Patients often describe the pain as dull, on one or both sides, with sharp flare-ups of pain. Pain with intercourse is common, too, often with discomfort afterwards.
As a general rule, women with labial varicose veins are younger, carry less weight and have less pelvic fat tissue. In addition, their babies are bigger than women who have typical varicose veins in the legs. Thoughts are that having less pelvic fat may allow pelvic organs to compress the pelvic veins more. Thus forcing venous blood through the ‘escape points’ between the pelvis and the vulva, labia, perineum, buttocks and legs.
And the Treatment Options?
The cause of the vulval varicose veins will define the treatment. If related to pregnancy, most will settle after delivery and no specific treatment is necessary. Varicose veins at the top of the thigh, which are linked to pregnancy vulval veins, require well-fitted compression stockings designed especially for pregnancy.

If the pain within the vulval varicose veins doesn’t go away on its own, treatment may be ultrasound-guided sclerotherapy. This is where injection of a vein irritant solution causes vein closure. Occasionally, a local anaesthetic day procedure called embolisation is necessary. This can block off the abnormal veins feeding the pelvic varicose veins. With the troublesome veins closed, improved blood flow out of the pelvis reduces the pressure and any symptoms within the pelvis.

AI in Arterial Conditions
AI in Arterial Conditions: How Technology Enhances Diagnosis
What is Artificial Intelligence?
AI tells computers to do jobs that people would normally do. For example, AI can read x-rays. Machine learning (ML) uses AI to improve the results of these jobs.
ML using AI is now better than a human at working out if a mole is likely to be melanoma or not.
Medical specialists, like vascular surgeons, rely on a lot of X-rays and scans to make decisions. As a result, ML and AI are good for solving all sorts of artery and vein problems.
Working out a patient’s outcome from treatment
AI can work out the chances of a good or not so good outcome from minimally invasive treatment or surgery. A mix of statistical models can be used to work out the risks of treatment. This information is often available on a smartphone.
All of the information from a patient can be compared to information from a large number of patients with the same condition to get a better result. Every time this happens, the AI can learn a little bit more about the condition. All of this is similar to the way humans learn from experience.

What vascular conditions currently use AI?
Abdominal Aneurysms (AAA)
AI is beginning to be useful in arterial vascular conditions, such as AAA and carotid artery disease.
In AAA, it can gather information about the growth, shape and make up of an aneurysm and, based on this, it can then give an accurate prognosis and the risk of rupture profile. Once a patient’s risk is known, better treatment decisions are available, such as ongoing observation or repair.
AI is also used in designing the best-fit stent treatment for aneurysms, based on multiple biometric factors. As well, AI can predict how the stent will function over time and help predict any future problems.
3D printers are coming to the fore in creating body parts that mimic a patient’s own. For use in hip replacements and implants and also custom made stents for aortic aneurysms.

Carotid Artery Disease
The risk of having a stroke from a narrowing in the carotid artery increases as the narrowing closes more. There are certain features of carotid disease, also called plaque, that increase the risk of a stroke. Recent bleeding inside the plaque, and dimples on the surface lining of the artery, are examples of this.
Using all of this information, AI is proving useful in predicting whether someone is at increased risk of having a stroke. Once this risk is known, there can be better decisions about carotid treatment. For example, whether to just keep keep a close eye on the artery or whether to operate.
As well, if a patient has already had a stroke caused by the carotid artery, AI can improve decision- making about whether urgent surgery is needed or not.


Is being overweight a reason for your swollen legs? Where to now?
Leg Swelling and Obesity: Causes, Risks and Treatment Options
Obese people often have leg swelling. This arises from two main mechanisms. The first is high blood pressure in the veins, which causes a build up of fluid in the legs. The second is reduced mobility because of difficulty with everyday activities, such as walking and exercise.
Why is weight so difficult to control?
The answer to this question is complex. Strong evidence suggests a person’s natural weight is pre-set by the brain from an early age, making weight loss over time difficult.
In obese people, weight loss results in a decreased metabolic rate, that does not appear to return to normal rates. If anything, it continues to decrease over time. In other words, a person becomes more likely to convert calories to fat. It is as if the body is always trying to return that person to their pre-set obese weight.
Are hunger hormones to blame?
Also, a hormone called leptin, one of many similar hunger hormones, plays a big part. When leptin falls, appetite increases and vice versa. After weight loss, leptin levels fall but appear never to return to normal, making people feel hungry most of the time. Again, it’s the brain trying to return people to their pre-set obese weights.
What we do know is dieting and cutting calories are not the only answer for the majority of overweight people. This is because always being hungry, with a lower metabolic rate, win out in the end. It’s biology and not a lack of willpower.

Weight loss surgery is effective in controlling calorie intake and appetite but actual treatments for the underlying problem are still in their infancy.
What can I do about my leg swelling?
Obviously, calorie control, exercise and being a healthy weight are still important.
Increasing exercise helps with wellbeing, burns calories and helps the flow of fluid out of the legs.
Varicose veins treatment can help if the veins are causing symptoms. These may be aching or skin problems, such as discolouration, cellulitis, bleeding, ulcers or eczema caused by varicose veins. Although, as weight increases, the effectiveness of vein treatment decreases.
Wearing compression socks or stockings is the mainstay of treatment for most people. These reduce fluid building up over the day and encourage blood flow back to the heart.


What is a leg ulcer?
Leg Ulcers: Causes, Symptoms and Effective Treatments
A leg ulcer occurs when there is a loss of skin cover that lasts for longer than is normal.
What is the scale of the problem?
Leg ulcers are an increasing problem in New Zealand, affecting about 1.5% of the population. Much of the increase in ulcers is related to our ageing population and increasing rates of diabetes and obesity. So, in New Zealand that is around 75,000 people. Managing leg ulcers is costly for society and the health system, as well as causing much discomfort and nuisance for affected patients.
What are the risks of a leg ulcer?
Venous ulcers, that is, ulcers caused by varicose veins or deep vein problems, like blood clots, are the most common cause of leg ulcers. Having peripheral artery disease increases the risk of developing an arterial leg or foot ulcer. The risk of diabetic foot ulcers increases in people who have had poorly controlled diabetes for a long period of time.
What are the types of leg ulcer?
There are two broad categories of ulcer – leg ulcers and foot ulcers. In general, venous ulcers usually affect the legs, artery ulcers can affect the legs or the feet, and diabetic ulcers usually affect the feet.
Venous ulcers
Venous ulcers are the most common ulcers. Blood pools in the legs from varicose veins or deep vein problems, leading to leg swelling, oedema, dermatitis, discolouration, skin thickening and ulcers. All of these combine to impair healing.

Arterial ulcers
Poor artery flow to the legs from blocked arteries caused by peripheral artery disease (PAD), or some other artery condition, can cause artery ulcers. An ulcer forms when the skin breaks down and there is not enough blood supply to allow healing.
Often venous and arterial ulcers occur at the same time.

Diabetic foot ulcers
Diabetes may attack the nerves to the feet, resulting in loss of feeling and loss of the protective system that helps prevent injury and infection. Repeated injury to the foot skin increases the risk of ulcers. Artery disease risk is higher in people with diabetes and this compounds the problem.

What can be done?
Treating an ulcer will involve a multidisciplinary team of community nurses, GPs, diabetes specialists, skin specialists, vascular specialists, orthopaedic and plastic surgeons, podiatrists and wound care specialists.
First up, vascular investigations assess the arteries and veins with an ultrasound scan. X-ray and MRI scans are good for assessment of any underlying bone and tissue issues.
Varicose veins, deep vein problems, and artery problems will need to be managed.
Other medical issues, such as diabetes, high blood pressure, high cholesterol and obesity will all need addressing as well. Smoking increases ulcer risk and patients will be encouraged to give up.
Ulcer dressings are a specialised area of wound care and there are many different dressing options available. Special shoes worn to relieve pressure may also help those with foot ulcers. Compression socks or stockings are a vital part of patient care, because they help relieve pressure and can reduce swelling.